
Registered Nurse | Healthcare Experience Since 2009
Just like urinating, everybody has bowel movements (abbreviated as BM). It is a part of life and we should make sure it is happening correctly. The amount, consistency, and how often patients go will vary greatly but that doesn’t mean it shouldn’t be monitored.
Table of Contents
How Often?
How often should your patient go? Let me put it this way. I work at a hospital and one of the requirements in order for a patient to be discharged is they must have had a bowel movement within the past 48 hours.
It doesn’t matter how well they are doing, no stool, no discharge. You may think that’s ridiculous but that just goes to show you how often your patients should go. Constipation is not taken lightly.
Does that mean rush your patient to the emergency room if they haven’t gone in two days? Not necessarily. There are simpler things you can do to help relieve constipation.
Laxatives, stool softeners, enemas, or even simpler things such as prune juice, apple juice, and coffee are known to help people have a bowel movement. Some patients have me warm up prune juice because it makes it even easier to go.
It’s hard to say when you should take drastic measures like going to the emergency room because it’s different for everybody. I personally have a bowel movement at least once a day while other people I know go every two or three days.
If your patient has pain or discomfort and hasn’t had a bowel movement for longer than usual for them, take action. I would first recommend the simple things mentioned above and if that doesn’t work in a timely manner, the emergency room may be necessary. A small bowel obstruction (SBO) can be a serious matter.
Hemorrhoid
If your patient is constipated, they may push and push to have a bowel movement until they give themselves a hemorrhoid. If they feel pain or discomfort around their anus, check to make sure a hemorrhoid isn’t bulging out. If you don’t know what they look like, it will look red, purple, and bubbly. You will know one when you see one.
If you see one, there are hemorrhoid creams you can buy to help push them back in. If cream is not readily available, another method I have personally seen work, is to gently rub the bulging area until it sinks back into the anus. This may take a few minutes to work. If nothing is getting rid of it and it is causing your patient major pain, a trip to the emergency room may be necessary.
Diarrhea
At the other end of the spectrum, if your patient is going too much, that is also a problem. When this happens, the stool will be in liquid form or diarrhea as most people call it. When this happens they can dehydrate very quickly because fluids go right through them.
Of course there are medications your patient can take for that as well but more importantly, you should make sure they drink plenty of fluids. If they can’t keep fluids down, you should take them to the emergency room where they can stay hydrated through IVs.
Clostridium Difficile (C diff)
Don’t try to pronounce the word above, just call it c-diff. What is it exactly? It is the worst kind of diarrhea caused by antibiotics and it is also becoming more and more common.
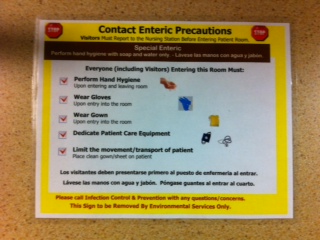
Working at a hospital, this is one of the most contagious bacteria I come into contact with and that’s saying a lot. The hospital knows this so we put patients with it on a special kind of contact precautions called contact enteric precautions.
Before you come into contact with a patient with c-diff, perform your handwashing duties, put on an isolation gown, and double up on medical gloves. After you are done, throw everything with the bacteria on it in the medical waste bin and immediately wash your hands again. Hand sanitizer will not kill it.
If you think your patient may have this bacteria and haven’t done so yet, take them to the emergency room so they can get immediate assistance. Then, make sure you scrub everything your patient came into contact with at home with bleach. Believe it or not, the bacteria can live on uncleaned surfaces for up to 70 days.
How will you know if your patient has it? If they have a mild case, it can be hard to tell but if they have a serious case, it is very easy to tell. It has a very unique and strong smell that you will never forget once you smell it for the first time. Sometimes it is also slightly yellow and/or light green in color.
There is actually an assessment tool that we use at the hospital to determine if it is necessary to send a stool specimen to check for c diff. If the patient meets these three criteria, then it is recommended to send a specimen to the lab for further evaluation.
- Patient has diarrhea of three or more stools in the last 24-36 hours.
- Stool consistency is equivalent to Bristol Stool Chart Type 6 or 7 (see below).
- Patient has not received laxatives or other medications causing diarrhea in the last 2 days.
What Does It Look Like?
When any of my patients have a bowel movement, I have to document when they had one regardless if they are on strict I & Os or not. I also have to describe what it looked like. The qualities I list are the:
- amount: small, medium, or large. Either is preferred but the less they go, the more often they should go.
- color: brown, green, yellow, or red which would mean blood is in the stool. Brown is preferred.
- consistency: formed, hard, loose, or liquidy. Formed is preferred. See the bristol stool chart below.
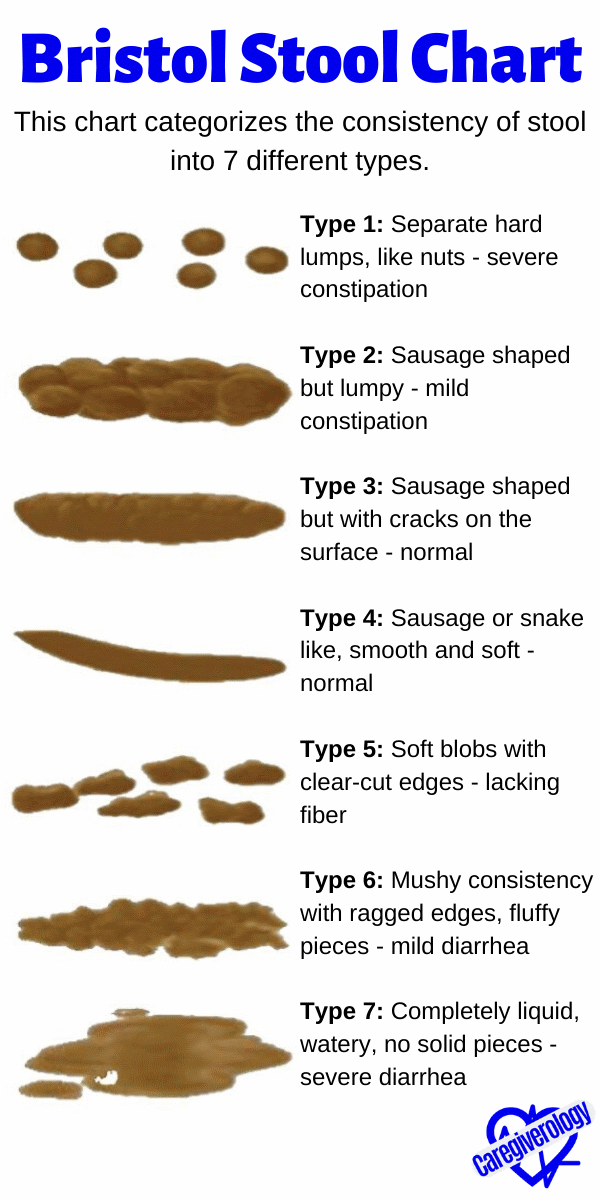
Bristol Stool Chart
This chart categorizes the consistency of stool into 7 different types.
Type 1: Separate hard lumps, like nuts – severe constipation
Type 2: Sausage shaped but lumpy – mild constipation
Type 3: Sausage shaped but with cracks on the surface – normal
Type 4: Sausage or snake like, smooth and soft – normal
Type 5: Soft blobs with clear-cut edges – lacking fiber
Type 6: Mushy consistency with ragged edges, fluffy pieces – mild diarrhea
Type 7: Completely liquid, watery, no solid pieces – severe diarrhea
Click here for a poster of this chart

Stool Specimen
If you work at a hospital like me, you may be asked to collect a stool specimen. To do that, use a “hat”, which is an item you place in a toilet or bedside commode to catch stool or urine. You could also collect it from a bedpan if your patient is on bedrest. Just make sure the stool is not mixed with urine.
You should then use a tongue depressor or spoon to scoop some of the stool into a container. You don’t need much, just a spoonful or two. Then put that patient’s label on the container with the time, date, and your name or initials on it. Then take it to the laboratory in a tiny biohazard bag within the next few hours.
Bowel movement specimens usually last a little longer than urine specimens which are only good for two hours. All of these things must be done in order for the specimen to be accurate.
Save This Guide
.%20It%20is%20a%20part%20of%20life%20and%20we%20should%20make%20sure%20it%20is%20happening%20correctly.%20%23caregiverology%20%23bowelmovement%20%23stool%20%23feces)